
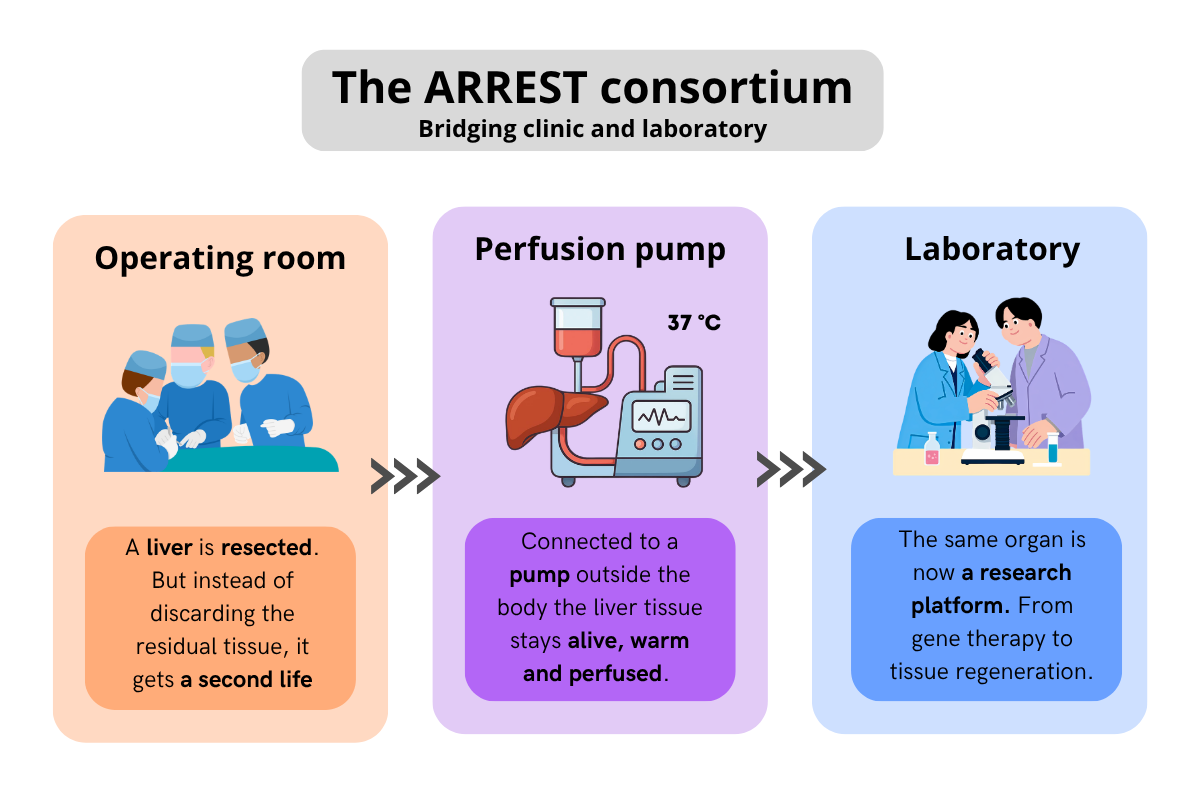
A human liver kept alive outside the body, perfused and tested, repaired and perhaps one day regrown. This vision is driving the ARREST Consortium, which received a major grant of €6.75 million. A Dutch multi-center collaboration that wants to bridge laboratory discovery and clinical reality.
Every year, hundreds of patients in the Netherlands wait for a liver transplant that may never come. Treatments available for severe liver disease remain limited and due to the lack of sufficient and good quality donor livers about 15% of patients currently die whilst on the liver transplant waiting list. It is against this backdrop that the ARREST Consortium, a collaboration of nearly all Dutch transplantation centers, has been established with a bold ambition: to use the human liver itself as a research model. "The idea is that we want to further develop the liver on a pump, perfused at near physiological conditions outside the body, as a research model," explains the consortium's coordinator Stan Van De Graaf, liver-scientist and head of the Tytgat Institute at Amsterdam UMC.
A unique human model
What makes the ARREST Consortium stand out is the nature of the model itself. Research on liver biology has traditionally relied on pig livers, cell lines, mouse models or organoids. Each has its advantages, but none comes close to the real thing. "This is by far the closest to a human liver in vivo," says Stan. "Even though it is not the natural state of a liver to be outside the human body, we still believe it is a very good model. It is already known that a liver can be preserved outside the body for quite some time on a pump system and then still be transplanted successfully." Importantly, ARREST relies primarily on residual tissue that would otherwise be discarded, making the approach both practical and resource-efficient.
The perfusion technology that makes this possible is in itself a Dutch success story. From the pioneering work on cold perfusion to normothermic perfusion, where the organ is kept at 37 °C and continues to function, the Netherlands has been at the forefront. "In the Netherlands, virtually all transplantations are now performed using this technology," notes one of the consortium's surgeons Joris Erdmann from Amsterdam UMC. The ability to test an organ during perfusion has been transformative. Traditionally, one current measure to determine liver disease involves clinicians physically assessing the density and macroscopic aspect during the procurement procedure. Instead of relying on this subjective approach, clinicians can now measure biochemical parameters, such as bile composition and pH values during perfusion to more accurately assess whether an organ will function successfully after transplantation.
From transplantation to oncology and beyond
The consortium spans seven work packages, covering topics from bile duct repair to gene editing, cell therapy to liver regeneration. But one of the most striking aspects is the contribution from oncological liver surgery. Joris Erdmann: "When we remove part of a patient's liver because it contains a tumor, the remaining half needs to take over full function. If we can grow that remaining liver larger beforehand, we can perform bigger operations or reduce the risk for the patient."
The resected portion offers a valuable opportunity. Kept alive on the perfusion machine, it becomes a platform for cancer research. "You also keep the tumor alive," Joris explains. "So you have a beautiful model for cancer research, as good as it gets, before you apply anything to patients. You could look at tumor-specific drug development, or mechanical therapies like ablation, and you can see exactly what damage is being done to the surrounding tissue."
This vision points towards personalized medicine: rather than giving every patient the same chemotherapy and waiting three months for a scan to find out whether it is working, future patients might have their tumor quickly tested ex vivo. "You could test whether certain combinations work for this specific patient," he says. "That would be a truly enormous step forward."
"You could test whether certain combinations work for this specific patient," he says. "That would be a truly enormous step forward."
The challenge of liver regeneration
Among the most ambitious goals in the consortium is understanding, and ultimately stimulating, liver regeneration. The liver is already uniquely capable of regrowth in vivo: after a partial resection, the remaining tissue rapidly expands to restore full function. But translating that capacity to an ex vivo perfusion system is uncharted territory.
"In the body, regeneration happens naturally. But this is not happening yet in the current perfusion system. So, we ask ourselves: is there a factor present in the pump system that is inhibiting regeneration or can we add a factor that is now missing?", reflects Stan. "I think it is more likely that something is absent. The perfusate we work with is quite minimal in composition. I have hope that by adding a handful of factors, we will start to see something."
Although ideal, the first milestones would not be livers physically growing in a dish: that remains science fiction for now. Instead, the first signs of progress would be microscopic: increased cell division, measurable markers of hepatocyte proliferation. "If we can see those first steps, I think the whole world will start tinkering with this," says Stan, "and it will get better and better. Until at some point, you really do see a liver beginning to grow physically in the system."
The timescales are encouraging: regeneration in the human body happens over days to weeks, exactly the window that current perfusion systems can maintain a liver ex vivo. "When I put those two things together," Stan explains, "it at least seems to be worth trying."
The logistics of a scarce resource
Ambitious science requires careful logistics. The consortium draws on several types of liver tissue, yet the numbers are modest. "If we manage to get ten resected livers onto the pump per year, that would already be a major achievement," estimates Joris. "Realistically, it might be five." This scarcity drives innovation: the work is organized to make the most of each team’s expertise.”
Before the biology research can begin, however, logistical and regulatory groundwork must be laid: pathology teams need to complete their diagnostic work, ethical approval must be navigated, and the infrastructure for connecting a partial liver to a perfusion machine must be built from scratch. "Getting all of that to work will already be an enormous achievement," says Joris. "Once it runs, we can do anything."
From lab to patient: a shared effort
The ARREST Consortium runs for six years, a timeline the team believes they will need, given the low annual volumes and the gradual process of building a new research platform. It brings together Dutch transplantation centers of Rotterdam, Groningen and Leiden, and is complemented by liver scientists from Utrecht, Leiden and Amsterdam. Work packages are deliberately distributed across multiple locations to increase organ availability, expertise and encourage collaboration.
"This is not a project that lends itself to being cut into separate pieces, with everyone just continuing their own research," Stan acknowledges. "The Netherlands is actually a beautiful country for this kind of work. Small enough that people understand they need each other, but large enough to have real expertise distributed across different centers."
Patient organisations including the Dutch Liver Patients Association (NLV) and VKS, but also other societal organisations such as Metakids and MDL Foundation are embedded in the consortium's board. Their response has been enthusiastic, VKS and Metakids particularly for work packages focused on gene therapy and cell therapy, where the path from laboratory discovery to clinical application has historically been long and frustrating. "They see this as a beautiful bridge," says Stan, "because with CRISPR (a gene-editing technology that allows scientists to precisely modify DNA), the discoveries came fast, but translating them into something that helps patients has turned out to be genuinely hard. We think this model can help change that."
"What I often hear from patients," says Joris, "is that it gives meaning to contribute to science. You are confronted with a serious illness, and you see that the treatments available today came from earlier patients who participated in research. They want to be part of that chain.
Patients themselves are also motivated to contribute. "What I often hear from patients," says Joris, "is that it gives meaning to contribute to science. You are confronted with a serious illness, and you see that the treatments available today came from earlier patients who participated in research. They want to be part of that chain." In that sense, contributing to ARREST is a relatively accessible way for patients to support the next generation of treatments.
Ten years from now
Asked to describe their most realistic ideal outcome in a decade's time, both researchers speak with measured but genuine optimism.
"I would love to see the liver on the pump being used for all these different applications in both the transplantation and research setting, and for this to have spread across the world, partly because of what this consortium has launched," says Stan. "Sharing the technology openly, not shielding expertise from others. The potential is too big for that."
Joris’s vision is even more vivid: "I hope that in ten years we are doing living-donor liver transplantation where we take a very small piece of the donor's liver, send it to a growth facility, and it comes back in a box. By courier, one minute before we need to put it in. And if the first one doesn't work, we grow a spare."
Science fiction, perhaps for now. But science fiction built on a foundation of real biology, real livers, and a group of researchers who are working on a problem they have decided to share.
Authors
Thalia Moedersheim
Ana Avramovic
Femke Mol